Ultrasound Tech Salary: What Your Certification Specialty Is Really Worth (And Why Most Techs Leave Money on the Table)

Your credentials matter more than your experience, and you’re probably getting underpaid. Contract positions pay more but the math is trickier than recruiters admit. Part-time gigs often beat full-time on an hourly basis. And your resume might be costing you $10K+ before you even get to the negotiation table.
Why Your Registry Credential Matters More Than Your Years of Experience
A two-year tech just got hired at $18,000 more than the ten-year veteran sitting next to her. Same shift. Same hospital. The only difference? Three letters on her certification.
Get your experience. Put in your time. Watch your salary climb. That’s the advice everyone gives, and for most healthcare jobs, it’s true. For ultrasound? It’s garbage.
I’ve been recruiting for imaging departments for eight years, and I’m going to tell you exactly what we look for when we’re deciding between the $72K offer and the $88K offer. It’s not your years of experience. It’s not your glowing references. It’s the specific registry credentials you hold.
Hospitals structure their pay scales around what you’re legally and technically qualified to do, not how long you’ve been doing something adjacent to it. According to the U.S. Bureau of Labor Statistics, sonographers earn a median annual salary of $89,340, but this number hides everything interesting. The top 10% pull $123,170 while the bottom 10% make $64,760. That’s not a small gap—that’s a different life.
The Credential Hierarchy That Determines Your Bracket

ARDMS has a bunch of different credentials, and they’re not created equal when it comes to your paycheck.
General sonography credentials (RDMS with OB/GYN or abdominal concentrations) are your baseline. Positions pay $62,000 to $78,000 in most metro markets. Nothing special, nothing terrible.
Cardiac sonography (RDCS) immediately bumps you into the $75,000 to $95,000 range. Vascular technology (RVT) sits similarly high. The reason? Scarcity—facilities need these skills but can’t easily cross-train their general sonographers to fill the gaps. Supply and demand isn’t just economics class theory.
Sarah had eight years of OB/GYN experience at a community hospital, pulling $74,000 annually. Solid reviews. Patients loved her. She knew that hospital inside and out. Then Marcus joined the cardiac unit. This 26-year-old kid who still wore Vans to work had just two years of general sonography experience but a fresh RDCS credential. His starting salary? $86,000.
Sarah went home that day and rage-applied to every cardiac sonography program in the state. Took her 14 months—but she got the cert. Now she makes $91K and Marcus asks HER for advice.
Pediatric (RMSKS for musculoskeletal) and breast sonography credentials occupy niche spaces with their own premium pricing. We’re talking $5,000 to $12,000 above general rates in markets where these specialties are in demand.
Why Experience Alone Won’t Bridge the Gap
You might spend a decade performing OB ultrasounds with exceptional skill. That experience is valuable, but it doesn’t credential you to perform echocardiograms. Hospitals can’t legally or practically slot you into cardiac positions regardless of your tenure.
Experience hits a ceiling—your tenth year as a general sonographer might earn you $82,000 while someone’s third year as a cardiac sonographer pulls $88,000. The market doesn’t care about fairness in this equation. It cares about credentialed capability and replacement cost.
Your certification roadmap matters more than your employment longevity. Planning which credentials to pursue based on market premiums will impact your lifetime earnings far more than loyalty to a single employer or specialty. The ultrasound tech salary you command depends on strategic choices you make about which credentials to pursue, not just how many years you’ve been scanning.
The Hidden Salary Tiers Nobody Talks About During Training
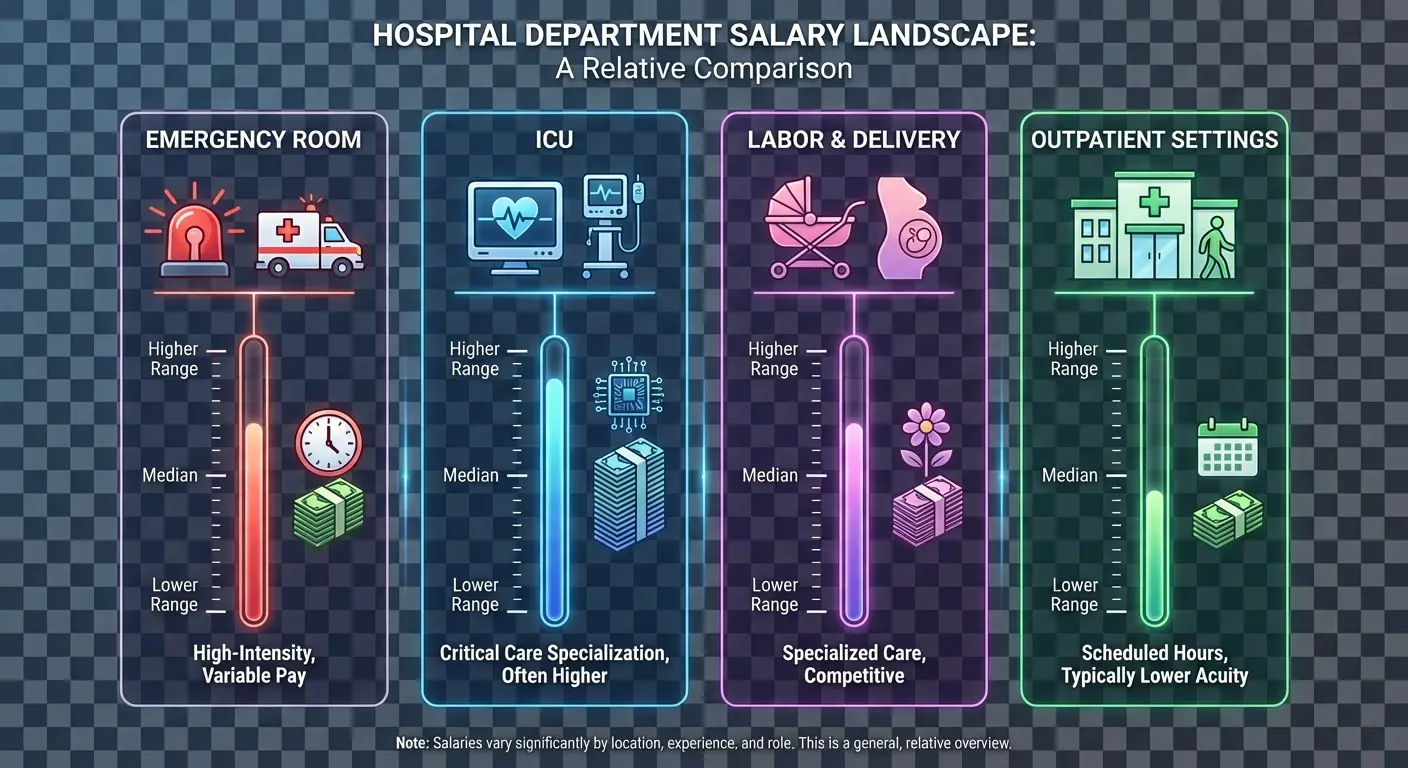
Your training program taught you anatomy, physics, and scanning protocols. Did anyone mention that ER sonographers at the same hospital make $12 per hour more than their outpatient counterparts with identical credentials?
These internal tiers exist at virtually every multi-department facility. They’re not advertised in job postings—they don’t show up in salary surveys. You discover them through conversations with colleagues or (more painfully) when you realize you’re underpaid relative to the tech who transferred to a different floor.
Department Assignment as Salary Multiplier
Emergency department ultrasound positions command premiums for several reasons—higher acuity, faster turnaround demands, more unpredictable workflows. Facilities compensate for the stress and skill required.
ICU-based sonographers often earn similar premiums. You’re performing bedside studies on critically ill patients, working around ventilators and lines, adapting your technique to challenging circumstances. That flexibility and clinical judgment gets priced into your compensation.
| Department Type | Typical Hourly Premium vs. Baseline | Annual Salary Impact | Key Differentiators |
|---|---|---|---|
| Emergency Department | +$8-12/hour | +$16,640-24,960 | High acuity, rapid turnaround, unpredictable volume |
| ICU/Critical Care | +$7-10/hour | +$14,560-20,800 | Bedside portability, critically ill patients, equipment navigation |
| Labor & Delivery | +$4-7/hour | +$8,320-14,560 | 24/7 coverage needs, time-sensitive procedures |
| Outpatient Imaging | Baseline ($28-38/hour) | $58,240-79,040 | Scheduled appointments, stable workflows, predictable census |
| Mobile/Float Pool | +$5-8/hour | +$10,400-16,640 | Multi-department flexibility, variable assignments |
Outpatient imaging centers typically pay at the lower end of the scale—scheduled appointments, stable patients, predictable workflows. Less chaos means less compensation. You might prefer that environment (plenty of techs do, and I get it), but you should know it costs you $8,000 to $15,000 annually in most markets.
Shift Differentials That Actually Matter
Night shift differentials for ultrasound techs range from laughable ($1/hour) to genuinely lucrative ($8-10/hour). The difference depends on whether you’re working at a facility that truly struggles to staff overnight coverage.
Weekend premiums follow similar patterns. Some hospitals offer an extra $3/hour for weekend shifts. Others, desperate for weekend coverage in their ER or labor and delivery units, offer $10-12/hour premiums plus every other weekend off.
Calculate these differentials across your annual hours. A $6/hour night differential across 2,080 hours equals $12,480 in additional gross income. That’s real money—that’s a car payment, student loan acceleration, or investment account funding.
Cross-Departmental Credentialing Creates Leverage
Facilities will pay you more if you can flex between departments based on demand. An RDMS who’s also competent in vascular studies becomes infinitely more valuable than someone who only performs OB scans.
This isn’t necessarily about holding multiple registry credentials (though that helps, which we’ll cover next). Sometimes it’s just about demonstrating cross-departmental competency that gives schedulers flexibility. You become the tech they can’t afford to lose because you solve multiple staffing problems.
Jennifer worked as a general sonographer in the outpatient clinic at $32/hour for three years. When staffing shortages hit the hospital’s vascular lab, she volunteered to cross-train during her off-hours. After demonstrating competency in carotid duplex and venous mapping studies, her manager created a “hybrid” position for her: three days in outpatient, two days in vascular.
Her new base rate—$41/hour. A $9/hour increase that translated to $18,720 more annually. She didn’t earn a new credential. She just proved she could solve problems in two departments instead of one.
Some facilities formalize this with “float pool” positions that pay $5-8/hour premiums. Others just quietly compensate their versatile techs better during annual reviews. Either way, your willingness and ability to work across departments translates directly to salary growth. Understanding the ultrasound technician salary structure within your facility means recognizing these hidden tiers and positioning yourself to access them.
How Modality Stacking Transforms Your Earning Potential
Most techs think about additional certifications as additive. You make X with your RDMS, maybe you’ll make X + Y if you add an RVT.
The actual math doesn’t work that way.
Modality stacking creates multiplicative value because you’re solving a facility’s staffing puzzle in ways that single-credential techs can’t. And honestly—if you’re not willing to get at least one additional cert, you’re not serious about maximizing your earning potential. That might sound harsh, but I’ve watched this play out too many times.
The Scarcity Premium of Multi-Credentialed Techs
Facilities post jobs for “RDMS/RVT” or “RDCS/RVT” because they desperately need someone who can cover both areas. When they find you, they’re not just filling one position. They’re solving two staffing headaches with a single hire.
That relief has a price tag.
Multi-credentialed techs routinely negotiate salaries 15-25% higher than the posted range because their scarcity gives them leverage. You’re not competing against every sonographer in the market. You’re competing against the tiny subset who hold your specific combination.

I’ve seen RDMS/RVT techs in mid-sized markets command $95,000 when single-credential RDMS positions pay $72,000 and RVT positions pay $78,000. The combination premium exceeds either individual credential’s ceiling.
Strategic Sequencing of Additional Certifications
Your first credential gets you employed. Your second credential should target the highest market premium relative to study investment.
Before pursuing additional credentials, evaluate:
- Current salary vs. projected salary with new credential (aim for $12K+ increase minimum)
- Local market demand (check job postings for credential combinations in your area)
- Study time required (200-400 hours for most additional certifications)
- Exam and application costs ($200-600 depending on credential)
- Annual registry maintenance costs ($150-250 per credential)
- CE credit requirements (30-50 hours every 3 years per credential)
- Content overlap with existing knowledge (vascular overlaps significantly with general sonography)
- Timeline to certification (6-18 months realistic for most working techs)
- Employer tuition assistance or reimbursement availability
- Contract or commitment requirements if employer funds your education
For most general sonographers, adding vascular (RVT) offers the best return. The material overlaps significantly with what you already know, the exam has a reasonable pass rate, and the market premium is substantial. You’re looking at 6-12 months of focused study for a potential $15,000+ salary increase.
Cardiac (RDCS) requires more intensive study if you’re coming from general sonography, but the payoff matches the effort. Markets with strong cardiology programs will pay top dollar for RDMS/RDCS combinations.
Breast sonography and musculoskeletal certifications work better as third additions in specific markets. They’re valuable, but the universal demand isn’t there the way it is for vascular and cardiac.
Understanding how to ask for a raise becomes crucial once you’ve earned additional credentials and need to renegotiate your compensation.
When More Credentials Stop Making Financial Sense
You can overcredential yourself relative to available positions. Holding RDMS, RVT, RDCS, and RMSKS certifications is impressive, but you’re unlikely to find positions that utilize all four enough to justify the maintenance costs and continuing education requirements.
Each credential requires registry fees, CE credits, and periodic reexamination—that’s time and money. If you’re not actively using a credential or getting compensated for holding it, you’re just paying maintenance on unused credentials. Credential maintenance fees are basically a subscription service for your career—thanks, I hate it.
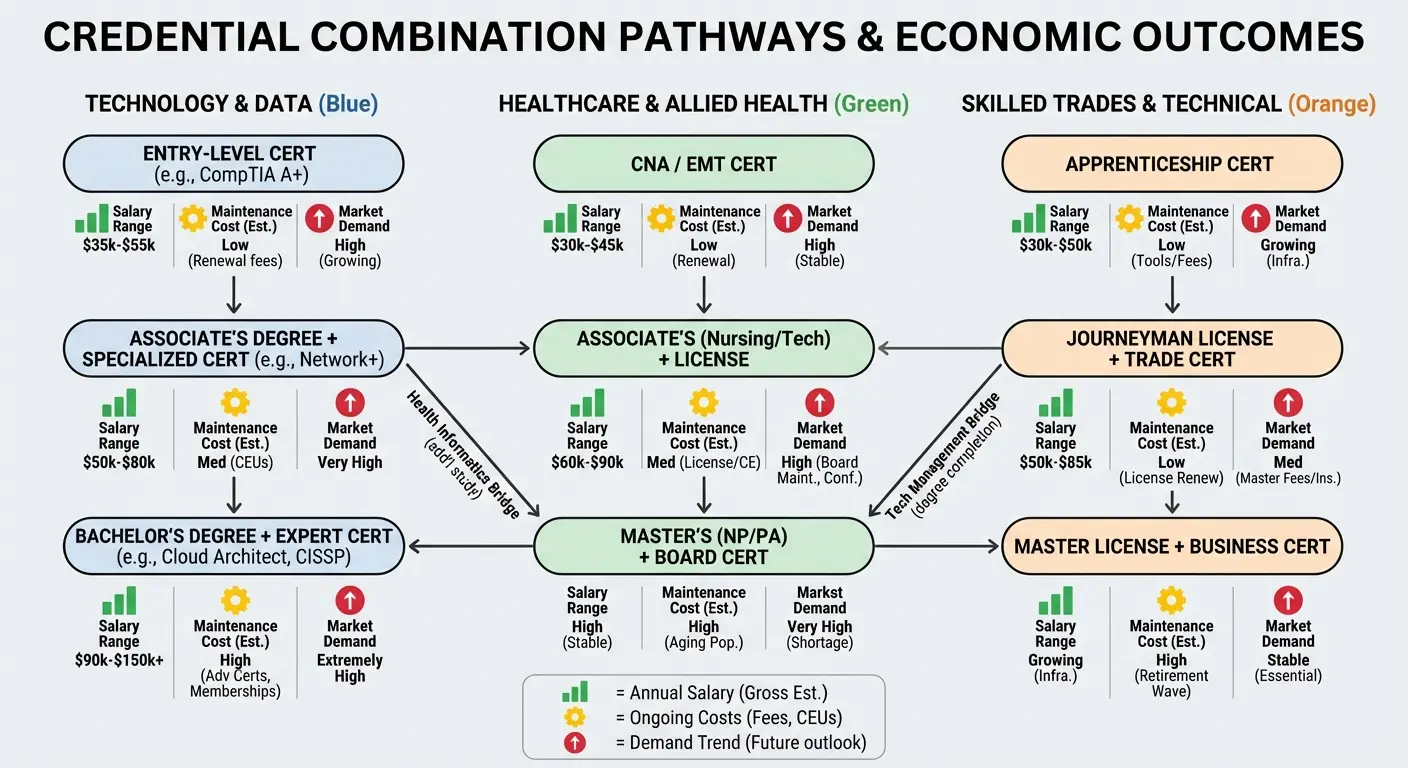
| Credential Combination | Typical Salary Range | Annual Maintenance Cost | Market Availability | Best For |
|---|---|---|---|---|
| RDMS only | $62,000-78,000 | $200 | Abundant | Entry-level, OB/GYN focus |
| RDMS + RVT | $78,000-95,000 | $400 | High demand | Maximum ROI for general sonographers |
| RDMS + RDCS | $82,000-98,000 | $400 | High demand | Cardiac-focused facilities |
| RVT + RDCS | $85,000-102,000 | $400 | Moderate | Specialized vascular/cardiac centers |
| RDMS + RVT + RDCS | $95,000-115,000 | $600 | Limited positions | Large academic medical centers |
| Four+ credentials | $98,000-120,000 | $800+ | Very limited | Academic/teaching hospitals only |
The sweet spot for most techs is two to three credentials that complement each other and align with your local market’s needs. Strategic credential stacking is the single most powerful lever you have to increase your earning potential without relocating or changing careers entirely.
Geographic Arbitrage for Sonographers (Without Relocating)
You don’t need to move to San Francisco or Boston to capture some of their salary premiums. The ultrasound field offers several pathways to geographic arbitrage that most techs never explore.
Telehealth Sonography’s Geographic Loophole
Remote ultrasound interpretation services need credentialed techs to perform scans at partner facilities. You might live in Oklahoma but contract with a telehealth company that services hospitals in New York and California.
The compensation structure typically reflects the service location’s market rates, not your home address. You’re capturing a portion of what New York facilities pay for sonography services while your mortgage or rent reflects Oklahoma prices.
These positions aren’t widely advertised—you’ll find them through specialized healthcare staffing platforms or by directly approaching telehealth companies that offer diagnostic imaging services. The work is real, the model is proven, but the awareness among techs remains surprisingly low.
Mobile Sonography Routes and Regional Contracts
Mobile imaging companies need techs willing to travel to nursing homes, clinics, and small hospitals within a region. You might cover a 100-mile radius from your home base, performing scans at facilities that can’t justify a full-time sonographer.

These routes often pay $40-55/hour (compared to $28-38/hour for staff positions) because you’re providing your own transportation and dealing with variable site conditions. You’re essentially running a service route, and the compensation reflects that entrepreneurial element.
Regional contracts work similarly but typically involve longer assignments (4-13 weeks) at a single facility that’s short-staffed. You might take a three-month contract two hours from home, stay in extended-stay housing during the week, and return home on weekends. The pay premium (often 40-50% above staff rates) compensates for the disruption.
Calculating True Geographic Arbitrage Value
The hourly rate tells part of the story. You need to account for mileage, wear on your vehicle, lodging costs (if applicable), and the irregular schedule that many of these arrangements involve.
A mobile route paying $48/hour sounds great until you realize you’re driving 200 miles per day and working 10-hour shifts. Your effective hourly rate after vehicle costs might drop to $38-40/hour. Still better than many staff positions, but not the windfall it first appeared.
Regional contracts that include housing stipends or per diem payments offer cleaner math. If the facility is covering your lodging and meals, that $45/hour is mostly pure income above your normal living expenses. A 13-week assignment could net you an extra $15,000-20,000 after expenses, which you can bank, invest, or use to pay down debt. The diagnostic medical sonographer salary you earn through these arrangements can significantly exceed traditional staff positions when you run the actual numbers.
The Part-Time Premium That Full-Timers Don’t Know Exists
Full-time employment feels secure—benefits, predictable schedules, the psychological comfort of a “real job.” But you’re probably leaving $15-20/hour on the table.
Data from Allied Health Schools shows that sonographers working in outpatient care centers earn an average of $123,020 per year, significantly more than the $89,340 median for all sonographers. Many of these higher-paying positions are structured as part-time or per diem arrangements that facilities use to manage variable patient volumes.
Why Per Diem Rates Exceed Staff Rates
Facilities pay per diem and PRN sonographers $10-20/hour more than their full-time staff because they’re buying flexibility without commitment. No benefits package, no guaranteed hours, no PTO accrual. Just on-demand coverage when they need it.
You become their overflow valve. When their staff tech calls in sick, when patient volume spikes, when they need weekend coverage, they call you. That convenience costs them more per hour but saves them money overall compared to hiring another full-time position.
A staff sonographer making $35/hour might see per diem techs earning $48-52/hour for the same work. Sounds backward until you account for the total compensation package. The facility is still saving money by avoiding benefits costs that typically add 30-40% to base salary.
Strategic Part-Time Positioning Across Multiple Facilities
Savvy techs create their own premium compensation packages. You work 16 hours per week at Facility A as per diem, 12 hours at Facility B, and 8 hours at Facility C. You’re working 36 hours total but earning per diem rates across all three positions.
Your effective hourly rate might average $48-50/hour compared to the $35-38/hour you’d earn in a single full-time position. Annually, you’re grossing $90,000-95,000 for fewer hours than a full-time position that pays $72,000-78,000.
The downsides—you’re managing multiple schedules, you’re responsible for your own health insurance, and you have no PTO. But if you’re healthy, organized, and value the income premium over traditional benefits, the math works strongly in your favor.
I once worked with a tech who juggled four different per diem gigs. She had a color-coded calendar system that would make a project manager weep with joy. Made $112K working what amounted to 32-34 hours per week—the scheduling gave her migraines, but her bank account was healthy.
Use an after-tax salary calculator to compare your actual take-home pay between part-time and full-time scenarios, accounting for tax implications of benefits.
The Benefits Breakeven Calculation
You need to know your number—at what hourly rate does the part-time premium outweigh the value of full-time benefits?
Start with health insurance. If you’re paying $600/month for marketplace coverage that your employer would have provided, that’s $7,200 annually. Add the value of PTO (typically 15-20 days, worth $4,000-6,000 in lost wages), retirement matching (3-6% of salary, another $2,500-4,500), and other benefits.
You’re looking at $15,000-20,000 in total benefit value for a typical full-time position. If your part-time hourly premium generates more than that annually, you’re ahead financially.
A $13/hour premium across 1,500 annual hours (30 hours/week, 50 weeks) equals $19,500. That covers your benefits loss and puts you ahead. A $10/hour premium across the same hours ($15,000) leaves you roughly even. Anything less, and you’re taking a financial hit for the flexibility.
Your personal situation determines which side of this equation makes sense. Young, healthy, no dependents? The part-time premium probably wins. Family health insurance needs, desire for employer retirement matching, value placed on PTO? Full-time might pencil out better despite the lower hourly rate. The ultrasound tech salary you command in part-time arrangements often exceeds what full-timers earn on an hourly basis, but the total compensation picture requires careful analysis.
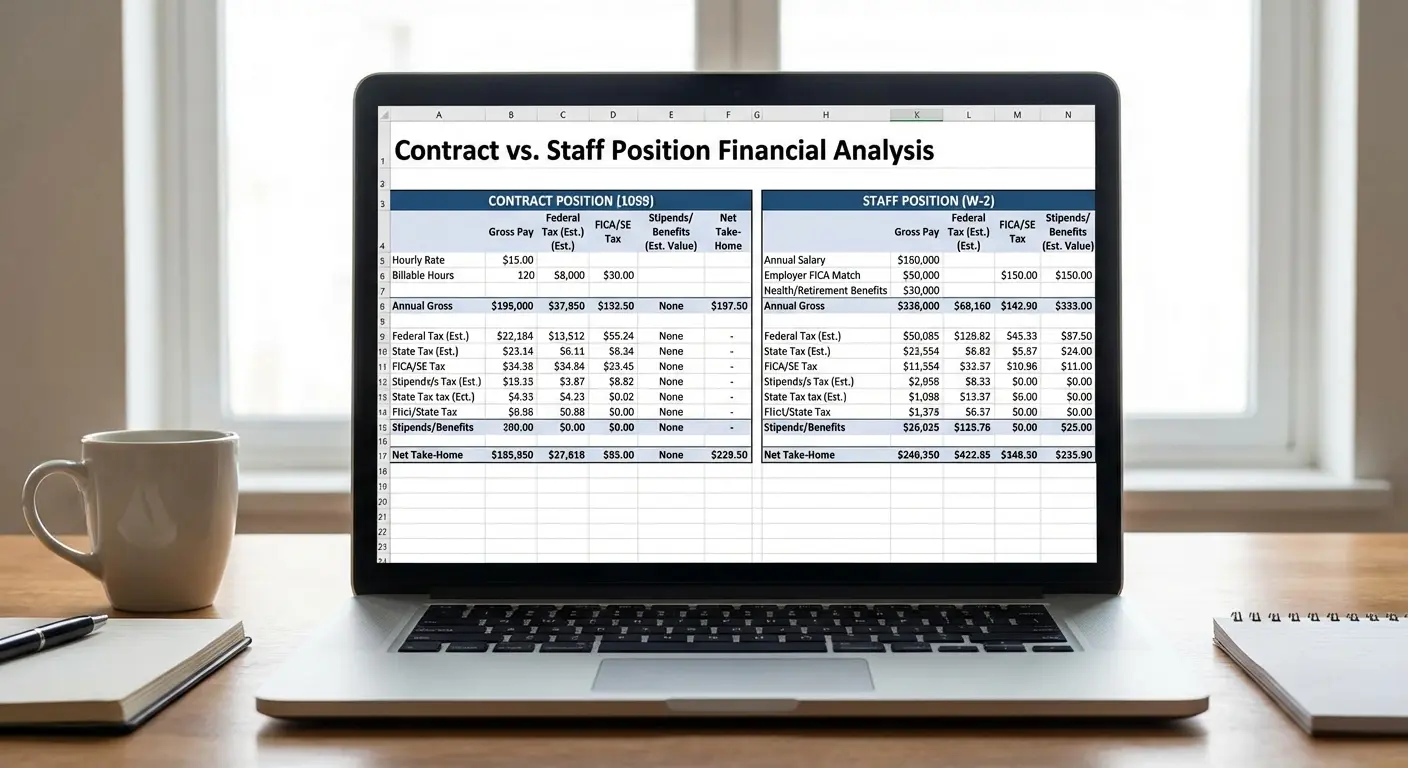
Contract vs. Staff: Running the Real Numbers
Those $3,500/week travel contracts look amazing until you actually do the math—and I mean the REAL math, not the math the recruiter shows you.
Your staff position pays $1,400-1,600 weekly. The choice seems obvious—except it’s not.
Deconstructing the Contract Pay Package
A typical contract might advertise “$3,200/week”—that breaks down to $32/hour taxable base rate (40 hours = $1,280) plus $1,920 in weekly stipends ($960 housing, $960 meals/incidentals).
The stipends are only tax-free if you maintain a permanent tax home elsewhere and you’re duplicating expenses. If you don’t have a mortgage or lease you’re maintaining back home, those stipends become taxable income. Your $3,200 weekly package just became $3,200 of fully taxable income, and your effective rate dropped significantly after taxes.
The whole “tax home” thing for travel contracts is byzantine—I’ve read the IRS guidelines three times and still don’t fully get it. Get an accountant if you’re going this route.
Even with legitimate tax-free stipends, you need to account for your actual housing and meal costs at the assignment location. If you’re spending $1,100/week on housing and food, your $1,920 stipend leaves you $820 ahead. Your real weekly gain is $1,280 (base rate) + $820 (stipend surplus) = $2,100, not $3,200.
The Gap Period Reality
Contracts end—you might line up your next assignment seamlessly, but most travelers experience 1-3 week gaps between contracts. Those are zero-income weeks.
Working 45 weeks annually instead of 50 weeks costs you five weeks of income. On a $3,200/week contract, that’s $16,000 in lost earnings. Your annual gross drops from $166,400 (52 weeks) to $144,000 (45 weeks). Still strong, but the gap matters.
Staff positions pay you 52 weeks regardless of patient census fluctuations or facility needs. That income reliability has value that doesn’t show up in hourly rate comparisons.
Contract work sounds sexy until you’re eating gas station sushi for the third time that week because you’re between assignments and trying to stretch your budget—ask me how I know.
Benefits Cost Transfer
Contract agencies offer benefits, but they’re rarely as comprehensive as hospital staff benefits. Your health insurance might cost $200-400/month in premiums with higher deductibles. Retirement matching is minimal or nonexistent. PTO doesn’t exist in the traditional sense.
You’re earning more hourly, but you’re also absorbing costs that staff positions include. A staff position offering $75,000 annually with full benefits might provide more financial value than a contract position grossing $95,000 but costing you $18,000 in benefits and gap periods.
The contract life works beautifully for techs who want geographic variety, can handle income variability, and are comfortable managing their own benefits. It works less well for techs who value stability, have family health insurance needs, or struggle with irregular income for budgeting purposes. Understanding the ultrasound technician salary structure in contract work means looking beyond the advertised weekly rate to the actual annual net income after all expenses.
Negotiation Leverage Points Specific to Ultrasound Tech Roles
You have more negotiation leverage than you think. Facilities need credentialed sonographers more than individual sonographers need any specific facility.
That power dynamic should inform every salary conversation you have.
Credential-Based Negotiation Anchors
Your certifications create objective value that transcends subjective performance discussions. When you’re negotiating initial offers, anchor to your credential combination, not to your years of experience.
“I’m seeing positions for RDMS-only techs in this market ranging from $68K to $74K. Given that I hold both RDMS and RVT certifications, I’m looking at the $82K to $88K range as a starting point for this conversation.”
You’ve just reframed the discussion around market value for your specific credential set, not around what they typically pay or what their budget allows. You’re forcing them to justify paying you less than market rate for your qualifications.
Imaging directors know credential scarcity. They know how hard it is to find multi-credentialed techs. They have budget flexibility they won’t advertise, but they’ll use it to secure candidates who solve multiple staffing needs.
Shift and Schedule Flexibility as Bargaining Chips
Your willingness to work nights, weekends, or rotating shifts has quantifiable value. Don’t give that flexibility away without compensation.

“I’m open to the evening shift, but I’d need to see that reflected in the base rate, not just the shift differential. What would the base salary be for an evening-dedicated position?”
Some facilities will adjust base pay for hard-to-fill shifts because shift differentials alone aren’t attracting candidates. Others won’t, but you’ll never know unless you ask. The worst they can say is no, and you’ve signaled that your flexibility has value.
Robert interviewed for a cardiac sonography position advertised at $78,000-84,000 for day shift. During negotiations, he mentioned he preferred evening shifts (3pm-11pm) due to childcare arrangements. The hiring manager came back with an evening-specific offer: $88,000 base salary plus a $4/hour evening differential. Robert’s willingness to work the hard-to-staff shift resulted in a $10,000 base salary increase above the posted range, plus an additional $8,320 annually from the differential. His total compensation reached $96,320, $12,320 more than the top of the advertised range, simply because he had flexibility the facility desperately needed.
Weekend-only positions sometimes offer premium base rates (think $5-8/hour above weekday rates) plus weekend differentials. You’re working 24 hours per weekend and getting paid for 40 hours, or you’re earning such a significant premium that 24 weekend hours equals 40 weekday hours in income. These arrangements exist, but facilities don’t advertise them. You have to negotiate them into existence.
The Annual Review Trap and How to Avoid It
Annual reviews at most facilities result in 2-4% raises. That’s not a negotiation—that’s cost-of-living theater.
Real negotiations happen during life changes for you or the facility. You completed a new certification? That’s a negotiation opportunity, not an annual review discussion. The facility is opening a new service line that needs your credentials? That’s leverage, and you should use it.
“I’ve completed my RVT certification and I know the vascular lab has been struggling with coverage. I’d like to discuss adjusting my compensation to reflect my expanded capabilities and the additional value I can provide to the department.”
You’re not asking for a raise. You’re proposing a compensation adjustment based on increased credentials and facility needs. The framing matters—you’re solving their problem, and you’re asking to be compensated appropriately for that solution. Your ultrasound tech salary should reflect your current credential set and market value, not what you were worth when you were first hired.
When Resume Builder IQ Becomes Your Salary Negotiation Tool
Your credentials have market value. Your resume’s job is to communicate that value clearly enough that you receive offers at the top of the range, not the bottom.
According to Best Colleges’ 2025 analysis, diagnostic medical sonography ranks among the top-earning associate degree careers, with median salaries of $82,570 placing it above most two-year degree professions. But only if candidates effectively communicate their specialized credentials and cross-modality competencies during the hiring process.
Most ultrasound tech resumes fail at this. They list ” RDMS, RVT” in a credentials section and hope hiring managers understand the implications—they don’t format their specialized competencies in ways that applicant tracking systems recognize. They undersell their cross-departmental experience because they don’t know how to present it effectively.
This costs you money before you ever get to the negotiation table.
How Credential Presentation Affects Initial Offers
Hiring managers and recruiters review dozens of sonographer resumes. They’re scanning for specific credential combinations and competencies. If your resume doesn’t highlight these elements immediately and clearly, you’re getting sorted into the general candidate pool instead of the specialized candidate pool.
That sorting determines your initial offer. General pool candidates get offers at the lower end of the range ($68K-72K). Specialized candidates who clearly demonstrate multi-modality competency get offers at the higher end ($78K-84K). Same credentials, different presentation—$10K+ difference in starting salary.
Resume Builder IQ helps you surface these critical elements in ways that both ATS systems and human reviewers recognize immediately. You paste in the job listing for an RDMS/RVT position, and the AI tailors your resume to emphasize your vascular competencies, relevant equipment experience, and cross-departmental capabilities that match what that specific facility needs.
You’re not changing your qualifications—you’re changing how effectively you communicate them, and that communication difference translates directly to better initial offers.
The Specialty Keyword Problem
Understanding resume keywords that get you hired is particularly crucial for sonographers, where specific modality terminology can mean the difference between an interview and an automated rejection.
Imaging departments use specific terminology in their applicant tracking systems. They’re filtering for “echocardiography,” “venous mapping,” “carotid duplex,” “strain imaging,” or other specialty terms that indicate advanced competency.
Your resume might say “performed cardiac ultrasounds.” Their ATS is looking for “transthoracic echocardiography” or “stress echocardiography.” You have the experience—your resume isn’t speaking their language.
This isn’t about keyword stuffing—different facilities and different specialties use specific terminology, and your resume needs to reflect that precision. An AI-powered resume builder that learns from actual job listings knows which terms matter for which positions and helps you present your experience using the language that gets recognized and valued.
If you’re sitting on valuable credentials but getting lowball offers, your resume presentation might be costing you thousands of dollars per year. Resume Builder IQ takes about 10 minutes to generate a tailored, ATS-optimized resume that communicates your credential value to the people making salary decisions. How much do ultrasound techs make? Often, it depends more on how effectively they present their qualifications than on the qualifications themselves.
Final Thoughts
The Bureau of Labor Statistics projects that employment of diagnostic medical sonographers will grow 13 percent from 2024 to 2034, much faster than the average for all occupations, with approximately 5,800 openings projected each year. This signals continued strong demand and negotiating leverage for credentialed professionals who strategically position themselves in the market.
As Middle Tennessee State University’s Allied Health program notes in their 2025 guidance, aspiring sonographers increasingly pursue bachelor’s degrees and multi-credential pathways rather than stopping at associate degrees, recognizing that advanced education and specialized certifications create measurably better career positioning and salary outcomes in an increasingly competitive healthcare market.
Your ultrasound tech salary isn’t predetermined by some industry standard or national average. It’s the result of specific choices you make about credentials, positioning, work arrangements, and negotiation strategies.

The techs earning $95K+ aren’t just lucky or more experienced. They’re strategically credentialed, they understand their market leverage, and they’ve structured their work arrangements to capture premiums that most techs don’t know exist.
Just as surgical tech salary strategies emphasize specialization and certification stacking, ultrasound technologists benefit from the same strategic credential approach to maximize earning potential.
Look, I’m probably biased here—I’ve spent nearly a decade watching techs undervalue themselves in negotiations, accept the first offer they get, and stay in positions that underpay them by $15K+ because they don’t realize what they’re worth. It drives me nuts.
You can follow the standard path. Get your RDMS, work staff positions, accept annual 3% raises, retire after 30 years. That’s a perfectly fine career—but if you want to accelerate your earnings, you need to think differently about how credentials compound, how work arrangements affect effective hourly rates, and how to position yourself for the opportunities that pay premium rates.
When evaluating sonographers pay structures across different employment models, remember that the highest earners aren’t necessarily working the most hours. They’re working the smartest arrangements. A sonographer salary reaches its full potential when you understand that compensation isn’t just about your clinical skills. It’s about strategic positioning in a market that desperately needs what you can provide.
The information is available—the pathways exist. Most techs just never look beyond the traditional employment model they learned about in school.
You don’t have to be most techs.